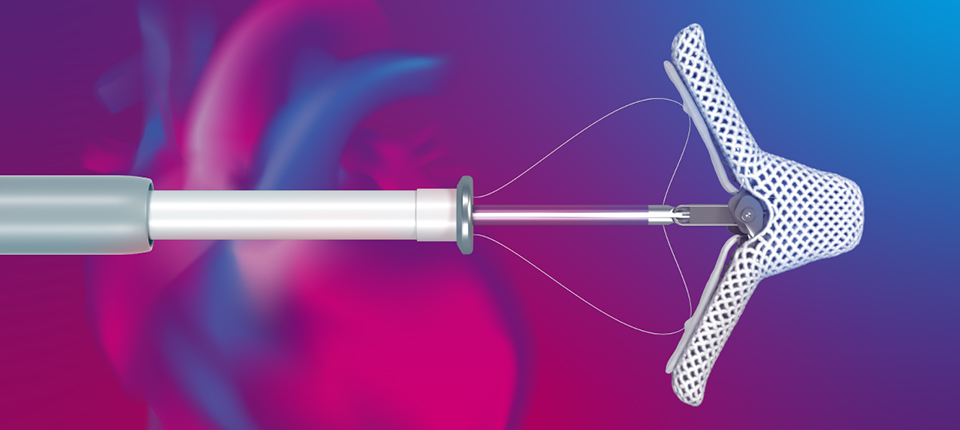
MITRACLIP CLIP DELIVERY SYSTEMS
MITRACLIP
INDICATION FOR USE • The MitraClipTM G4 System is indicated for the percutaneous reduction of significant symptomatic mitral regurgitation (MR ≥ 3+) due to primary abnormality of the mitral apparatus [degenerative MR] in patients who have been determined to be at prohibitive risk for mitral valve surgery by a heart team, which includes a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, and in whom existing comorbidities would not preclude the expected benefit from reduction of the mitral regurgitation. • The MitraClipTM G4 System, when used with maximally tolerated guideline-directed medical therapy (GDMT), is indicated for the treatment of symptomatic, moderateto-severe or severe secondary (or functional) mitral regurgitation (MR; MR ≥ Grade III per American Society of Echocardiography criteria) in patients with a left ventricular ejection fraction (LVEF) ≥ 20% and ≤ 50%, and a left ventricular end systolic dimension (LVESD) ≤ 70 mm whose symptoms and MR severity persist despite maximally tolerated GDMT as determined by a multidisciplinary heart team experienced in the evaluation and treatment of heart failure and mitral valve disease. CONTRAINDICATIONS The MitraClipTM G4 System is contraindicated in patients with the following conditions: • Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or post procedural anti-platelet regimen • Patients with known hypersensitivity to clip components (nickel / titanium, cobalt, chromium, polyester), or with contrast sensitivity • Active endocarditis of the mitral valve • Rheumatic mitral valve disease • Evidence of intracardiac, inferior vena cava (IVC) or femoral venous thrombus WARNINGS • DO NOT use MitraClipTM outside of the labeled indication. • The MitraClipTM G4 Implant should be implanted with sterile techniques using fluoroscopy and echocardiography (e.g. transesophageal [TEE] and transthoracic [TTE]) in a facility with on-site cardiac surgery and immediate access to a cardiac operating room. • Read all instructions carefully. Use universal precautions for biohazards and sharps while handling the MitraClipTM G4 System to avoid user injury. Failure to follow these instructions, warnings and precautions may lead to device damage, user injury or patient injury including: n MitraClipTM G4 Implant erosion, migration or malposition n Failure to deliver MitraClipTM G4 Implant to the intended site n Difficulty or failure to retrieve MitraClipTM G4 system components • Use caution when treating patients with hemodynamic instability requiring inotropic support or mechanical heart assistance due to the increased risk of mortality in this patient population. The safety and effectiveness of MitraClipTM in these patients has not been evaluated. • Patients with a rotated heart due to prior cardiac surgery in whom the System is used may have a potential risk of experiencing adverse events such as atrial perforation, cardiac tamponade, tissue damage, and embolism which may be avoided with preoperative evaluation and proper device usage. • For the Steerable Guide Catheter and Delivery Catheter only: n The Guide Catheter: the distal 65 cm of the Steerable Guide Catheter with the exception of the distal soft tip, is coated with a hydrophilic coating. n The Delivery Catheter: coated with a hydrophilic coating for a length of approximately 131 cm. n Failure to prepare the device as stated in these instructions and failure to handle the device with care could lead to additional intervention or serious adverse event. • The Clip Delivery System is provided sterile and designed for single use only. Cleaning, re-sterilization and / or reuse may result in infections, malfunction of the device and other serious injury or death. • Note the product “Use by” date specified on the package. • Inspect all product prior to use. Do not use if the package is open or damaged, or if product is damaged. PRECAUTIONS • Prohibitive Risk Primary (or degenerative) Mitral Regurgitation n Prohibitive risk is determined by the clinical judgment of a heart team, including a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, due to the presence of one or more of the following documented surgical risk factors: ◆ 30-day STS predicted operative mortality risk score of 4 ≥8% for patients deemed likely to undergo mitral valve replacement or 4 ≥6% for patients deemed likely to undergo mitral valve repair n Porcelain aorta or extensively calcified ascending aorta. n Frailty (assessed by in-person cardiac surgeon consultation) n Hostile chest n Severe liver disease / cirrhosis (MELD Score > 12) n Severe pulmonary hypertension (systolic pulmonary artery pressure > 2/3 systemic pressure) n Unusual extenuating circumstance, such as right ventricular dysfunction with severe tricuspid regurgitation, chemotherapy for malignancy, major bleeding diathesis, immobility, AIDS, severe dementia, high risk of aspiration, internal mammary artery (IMA) at high risk of injury, etc. n Evaluable data regarding safety or effectiveness is not available for prohibitive risk Primary patients with an LVEF < 20% or an LVESD > 60 mm. MitraClipTM should be used only when criteria for clip suitability for Primary have been met. n The heart team should include a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease and may also include appropriate physicians to assess the adequacy of heart failure treatment and valvular anatomy. • Secondary Mitral Regurgitation n Evaluable data regarding safety or effectiveness is not available for secondary MR patients with an LVEF < 20% or an LVESD > 70 mm. n The multidisciplinary heart team should be experienced in the evaluation and treatment of heart failure and mitral valve disease and determine that symptoms and MR severity persist despite maximally tolerated GDMT. POTENTIAL COMPLICATIONS AND ADVERSE EVENTS The following ANTICIPATED EVENTS have been identified as possible complications of the MitraClipTM G4 procedure. • Allergic reactions or hypersensitivity to latex, contrast agent, anaesthesia, device materials (nickel / titanium, cobalt, chromium, polyester), and drug reactions to anticoagulation, or antiplatelet drugs • Vascular access complications which may require transfusion or vessel repair including: n wound dehiscence n catheter site reactions n Bleeding (including ecchymosis, oozing, hematoma, hemorrhage, retroperitoneal hemorrhage) n Arteriovenous fistula, pseudoaneurysm, aneurysm, dissection, perforation / rupture, vascular occlusion n Emboli (air thrombotic material, implant, device component) n Peripheral Nerve Injury • Lymphatic complications • Pericardial complications which may require additional intervention, including: n Pericardial effusion n Cardiac tamponade n Pericarditis • Cardiac complications which may require additional interventions or emergency cardiac surgery, including: n Cardiac perforation n Atrial septal defect • Mitral valve complications, which may complicate or prevent later surgical repair, including: n Chordal entanglement / rupture n Single Leaflet Device Attachment (SLDA) n Thrombosis n Dislodgement of previously implanted devices n Tissue damage n Mitral valve stenosis n Persistent or residual mitral regurgitation n Endocarditis • Cardiac arrhythmias (including conduction disorders, atrial arrhythmias, ventricular arrhythmias) • Cardiac ischemic conditions (including myocardial infarction, myocardial ischemia, and unstable / stable angina) • Venous thromboembolism (including deep vein thrombosis, pulmonary embolism, post procedure pulmonary embolism) • Stroke / Cerebrovascular accident (CVA) and Transient Ischemic Attack (TIA) • System organ failure: n Cardio-respiratory arrest n Worsening heart failure n Pulmonary congestion n Respiratory dysfunction / failure / atelectasis n Renal insufficiency or failure n Shock (including cardiogenic and anaphylactic) • Blood cell disorders (including coagulopathy, hemolysis, and Heparin Induced Thrombocytopenia (HIT)) • Hypotension / hypertension • Infection including: n Urinary Tract Infection (UTI) n Pneumonia n Septicemia • Nausea / vomiting • Chest pain • Dyspnea • Edema • Fever or hyperthermia • Pain • Death • Fluoroscopy, Transesophageal echocardiogram (TEE) and Transthoracic echocardiogram (TTE) -related complications: n Skin injury or tissue changes due to exposure to ionizing radiation n Esophageal irritation n Esophageal perforation n Gastrointestinal bleeding.
Caution: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use provided inside the product carton (when available) or at eifu.abbottvascular.com or at medical.abbott/manuals for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. TM Indicates a trademark of the Abbott Group of Companies. www.Cardiovascular.Abbott
FREESTYLE LIBRE 14 DAY INDICATIONS AND IMPORTANT SAFETY INFORMATION
The FreeStyle Libre 14 day Flash Glucose Monitoring System is a continuous glucose monitoring (CGM) device indicated for the management of diabetes in persons age 18 and older. It is designed to replace blood glucose testing for diabetes treatment decisions. The System detects trends and tracks patterns aiding in the detection of episodes of hyperglycemia and hypoglycemia, facilitating both acute and long-term therapy adjustments. Interpretation of the System readings should be based on the glucose trends and several sequential readings over time. The System is intended for single patient use and requires a prescription.
CONTRAINDICATIONS: The FreeStyle Libre 14 day Flash Glucose Monitoring System must be removed prior to Magnetic Resonance Imaging (MRI), Computed Tomography (CT) scan, or high frequency electrical heat (diathermy) treatment. The effect of MRI, CT scans, or diathermy on the performance of the System has not been evaluated. The exposure may damage the Sensor and may impact proper function of the device which could cause incorrect readings.
WARNINGS:
Do not ignore symptoms that may be due to low or high blood glucose: If you are experiencing symptoms that are not consistent with your glucose readings, consult your health care professional.
Check Sensor glucose readings by conducting a fingerstick test with a blood glucose meter under the following conditions, when Sensor glucose readings may not be accurate and should not be used to make a diabetes treatment decision:
If you suspect that your reading may be inaccurate for any reason
When you are experiencing symptoms that may be due to low or high blood glucose
When you are experiencing symptoms that do not match the Sensor glucose readings
During the first 12 hours of wearing a FreeStyle Libre 14 day Sensor
During times of rapidly changing glucose (more than 2 mg/dL per minute)
When the Sensor glucose reading does not include a Current Glucose number or Glucose Trend Arrow
In order to confirm hypoglycemia or impending hypoglycemia as reported by the Sensor
When you see the Check Blood Glucose symbol, you must check your blood glucose with a blood glucose meter before making any treatment decisions. Sensor readings may not accurately reflect blood glucose levels.
Hypoglycemic unawareness: The System has not been evaluated for use in patients with hypoglycemic unawareness and will not automatically alert you of a hypoglycemic event without you scanning your Sensor.
No alarms without a Sensor scan: The System does not have alarms that will automatically notify you when you are having a severe low (hypoglycemic) or high (hyperglycemic) glucose event unless you scan your Sensor. For example, the System does not have an alarm that can alert or wake you when you are sleeping in the case of low or high glucose. Choking hazard: The FreeStyle Libre System contains small parts that may be dangerous if swallowed.
CAUTIONS AND LIMITATIONS:
Below are important cautions and limitations to keep in mind so you can use the System safely. They are grouped into categories for easy reference.
What to know about Alarms/Alerts:
There are NO alarms or alerts unless you scan the Sensor.
What to know before using the System:
Review all product information before use.
Take standard precautions for transmission of blood borne pathogens to avoid contamination.
Who should not use the System:
Do not use the System in people less than 18 years of age. The System is not approved for use in people under 18 years of age and Sensor readings in this population may be inaccurate. In general, continuous glucose monitoring systems are recognized to be less accurate in children than in adults.
Do not use the System in critically ill patients. The System is not approved for use in these patients. It is not known how different conditions or medications common to the critically ill population may affect performance of the System. Sensor glucose readings may be inaccurate in critically ill patients.
Do not use the System in pregnant women or persons on dialysis. The System is not approved for use in pregnant women or persons on dialysis and has not been evaluated in these populations.
Performance of the System when used with other implanted medical devices, such as pacemakers, has not been evaluated.
What should you know about wearing a Sensor:
The Sensor can be worn for up to 14 days.
Some individuals may be sensitive to the adhesive that keeps the Sensor attached to the skin. If you notice significant skin irritation around or under your Sensor, remove the Sensor and stop using the System. Contact your health care professional before continuing to use the System.
Intense exercise may cause your Sensor to loosen due to sweat or movement of the Sensor. Remove and replace your Sensor if it starts to loosen and follow the instructions to select an appropriate application site.
The System uses all available glucose data to give you readings so you should scan your Sensor at least once every 8 hours for the most accurate performance. Scanning less frequently may result in decreased performance.
Do not reuse Sensors. The Sensor and Sensor Applicator are designed for single use. Reuse may result in no glucose readings and infection. Not suitable for re-sterilization. Further exposure to irradiation may cause inaccurate results.
If a Sensor breaks inside your body, call your health care professional.
How to Store the Sensor Kit:
Store the Sensor Kit between 39°F and 77°F. Storage outside of this range may cause inaccurate Sensor glucose readings. While you don’t need to keep your Sensor Kit in a refrigerator, you can as long as the refrigerator is between 39°F and 77°F. Do not freeze.
Store the Sensor Kit between 10-90% non-condensing humidity.
When not to use the System:
Do NOT use if the Sensor Kit package, Sensor Pack, or Sensor Applicator appear to be damaged or already opened due to risk of no results and/or infection.
Do NOT use if Sensor Kit contents are past expiration date.
Do NOT use if the Reader appears to be damaged due to risk of electric shock and/or no results.
What to know before you Apply the Sensor:
The Sensor Pack and Sensor Applicator are packaged as a set (separately from the Reader) and have the same Sensor code. Check that the Sensor codes match before using your Sensor Pack and Sensor Applicator. Do not use Sensor Packs and Sensor Applicators with different Sensor codes together as this will result in incorrect glucose readings.
Clean the application site and ensure that it is dry prior to Sensor insertion. This helps the Sensor stay attached to your body.
Clean hands prior to Sensor handling/insertion to help prevent infection.
Change the application site for the next Sensor application to prevent discomfort or skin irritation.
Sensor placement is not approved for sites other than the back of the arm. If placed in other areas, the Sensor may not function properly.
Select an appropriate Sensor site to help the Sensor stay attached to the body and prevent discomfort or skin irritation. Avoid areas with scars, moles, stretch marks, or lumps. Select an area of skin that generally stays flat during normal daily activities (no bending or folding). Choose a site that is at least 1 inch away from an insulin injection site.
When is Sensor Glucose different from Blood Glucose:
Physiological differences between the interstitial fluid and capillary blood may result in differences in glucose readings between the System and results from a fingerstick test using a blood glucose meter. Differences in glucose readings between interstitial fluid and capillary blood may be observed during times of rapid change in blood glucose, such as after eating, dosing insulin, or exercising.
What to know about interfering substances such as Vitamin C and Aspirin:
Taking ascorbic acid (vitamin C) while wearing the Sensor may falsely raise Sensor glucose readings. Taking salicylic acid (used in some pain relievers such as aspirin and some skin care products) may slightly lower Sensor glucose readings. The level of inaccuracy depends on the amount of the interfering substance active in the body.
Test results did not indicate interference for methyldopa (used in some drugs to treat high blood pressure) or tolbutamide (infrequently used in some drugs to treat diabetes in the US) at maximum circulating levels. However, concentrations of potential interferents in interstitial fluid are unknown compared to circulating blood.
What to know about X-Rays:
The Sensor should be removed prior to exposing it to an X-ray machine. The effect of X-rays on the performance of the System has not been evaluated. The exposure may damage the Sensor and may impact proper function of the device to detect trends and track patterns in glucose values during the wear period.
When to remove the Sensor:
If the Sensor is becoming loose or if the Sensor tip is coming out of your skin, you may get no readings or unreliable readings, which may not match how you feel. Check to make sure your Sensor has not come loose. If it has come loose, remove it and apply a new one.
If you believe your glucose readings are not correct or are inconsistent with how you feel, perform a blood glucose test on your finger to confirm your glucose. If the problem continues, remove the current Sensor and apply a new one.
What to do if you are dehydrated:
Severe dehydration and excessive water loss may cause inaccurate Sensor glucose readings. If you believe you are suffering from dehydration, consult your health care professional immediately.
What to know about the Reader’s Built-in Meter:
The FreeStyle Libre 14 day Reader has a built-in blood glucose meter that is designed to be used only with FreeStyle Precision Neo blood glucose test strips and MediSense Glucose and Ketone Control Solution. Using other test strips with the Reader’s built-in meter will produce an error or cause the Reader’s built-in meter to not turn on or start a test. The Reader's built-in meter does not have ketone testing functionality.
The Reader’s built-in meter is not for use on people who are dehydrated, hypotensive, in shock, or for individuals in hyperglycemic-hyperosmolar state, with or without ketosis.
The Reader’s built-in meter is not for use on neonates, in critically-ill patients, or for diagnosis or screening of diabetes.
See Using the Reader’s Built-in meter section for additional important information on the use of the Reader’s built-in meter.
Where to charge your Reader:
Be sure to select a location for charging that allows the power adapter to be easily unplugged. Do NOT block access to the charger due to the potential risk of electrical shock.
FreeStyle Libre 2 Indications and Important Safety Information
Indications and Important Safety Information
The FreeStyle Libre 2 Flash Glucose Monitoring System is a continuous glucose monitoring (CGM) device with real time alarms capability indicated for the management of diabetes in persons age 4 and older. It is intended to replace blood glucose testing for diabetes treatment decisions, unless otherwise indicated.
The System also detects trends and tracks patterns and aids in the detection of episodes of hyperglycemia and hypoglycemia, facilitating both acute and long-term therapy adjustments. Interpretation of the System readings should be based on the glucose trends and several sequential readings over time.
The System is also intended to autonomously communicate with digitally connected devices. The System can be used alone or in conjunction with these digitally connected devices where the user manually controls actions for therapy decisions.
CONTRAINDICATIONS
Automated Insulin Dosing: The System must not be used with automated insulin dosing (AID) systems, including closed loop and insulin suspend systems.
MRI/CT/Diathermy: The System must be removed prior to Magnetic Resonance Imaging (MRI), Computed Tomography (CT) scan, or high-frequency electrical heat (diathermy) treatment. The effect of MRI, CT scans, or diathermy on the performance of the System has not been evaluated. The exposure may damage the Sensor and may impact proper function of the device which could cause incorrect readings.
WARNINGS
Before you use the FreeStyle Libre 2 System, review all the product instructions and the Interactive Tutorial. The Quick Reference Guide and Interactive Tutorial give you quick access to important aspects and limitations of the System. The User’s Manual includes all safety information and instructions for use. Talk to your health care professional about how you should use your Sensor glucose information to help manage your diabetes.
Failure to use the System according to the instructions for use may result in you missing a severe low blood glucose or high blood glucose event and/or making a treatment decision that may result in injury. If your glucose alarms and readings from the System do not match symptoms or expectations, use a fingerstick blood glucose value from a blood glucose meter to make diabetes treatment decisions. Seek medical attention when appropriate.
Do not ignore symptoms that may be due to low or high blood glucose: If you are experiencing symptoms that are not consistent with your glucose readings, consult your health care professional.
Use your blood glucose meter to make diabetes treatment decisions when you see the Check Blood Glucose symbol during the first 12 hours of wearing a Sensor, if your Sensor glucose reading does not match how you feel, or if the reading does not include a number.
Choking hazard: The System contains small parts that may be dangerous if swallowed.
CAUTIONS AND LIMITATIONS
Below are important cautions and limitations to keep in mind so you can use the System safely. They are grouped into categories for easy reference.
What to know about Glucose Alarms:
For you to receive alarms, they must be on and your Reader should be within 20 feet of you at all times. The transmission range is 20 feet unobstructed. If you are out of range, you may not receive glucose alarms.
To prevent missed alarms, make sure the Reader has sufficient charge and that sound and/or vibration are turned on.
Alarms you receive do not include your glucose reading so you must scan your Sensor to check your glucose.
What to know before using the System:
Review all product information before use.
Take standard precautions for transmission of blood borne pathogens to avoid contamination.
Make sure that your Reader and Sensor kits are kept in a safe place, under your control. This is important to help prevent anyone from accessing or tampering with the System.
Who should not use the System:
Do not use the System in people less than 4 years of age. The System is not cleared for use in people under 4 years of age.
Do not use the System if you are pregnant, on dialysis, or critically ill. The System is not cleared for use in these groups and it is not known how different conditions or medications common to these populations may affect performance of the System.
Performance of the System when used with other implanted medical devices, such as pacemakers, has not been evaluated.
What should you know about wearing a Sensor:
Wash application site on the back of your upper arm using a plain soap, dry, and then clean with an alcohol wipe. This will help remove any oily residue that may prevent the Sensor from sticking properly. Allow site to air dry before proceeding. Carefully preparing the site according to these instructions will help the Sensor stay on your body for the full 14 day wear period and help prevent it from falling off early.
The Sensor can be worn for up to 14 days. Remember to always have your next Sensor available before your current one ends so you can keep getting your glucose readings. You must scan the Sensor to get your real-time current glucose level as the Reader will not provide this information without a scan.
In the event that your Sensor stops working and you do not have another Sensor readily available, you must use an alternate method to measure your glucose levels and inform your treatment decisions.
The System is designed to detect certain conditions which may occur where the Sensor is not working as intended and shut it off, telling you to replace your Sensor. This may occur if the Sensor gets knocked off from the skin or if the System detects that the Sensor may not be performing as intended. Contact Customer Service if you receive a Replace Sensor message before the end of the 14 day wear period. Customer Service is available at 1-855-632-8658 7 Days a Week from 8AM to 8PM Eastern Standard Time.
Some individuals may be sensitive to the adhesive that keeps the Sensor attached to the skin. If you notice significant skin irritation around or under your Sensor, remove the Sensor and stop using the System. Contact your health care professional before continuing to use the System.
Intense exercise may cause your Sensor to loosen due to sweat or movement of the Sensor. If the Sensor is becoming loose or if the Sensor tip is coming out of your skin, you may get no readings or unreliable low readings. Remove and replace your Sensor if it starts to loosen and follow the instructions to select an appropriate application site. Do not attempt to reinsert the Sensor. Contact Customer Service if your Sensor becomes loose or falls off before the end of the wear period. Customer Service is available at 1-855-632-8658 7 Days a Week from 8AM to 8PM Eastern Standard Time.
Do not reuse Sensors. The Sensor and Sensor Applicator are designed for single use. Reuse may result in no glucose readings and infection. Not suitable for re-sterilization. Further exposure to irradiation may cause unreliable low results.
If a Sensor breaks inside your body, call your health care professional.
How to Store the Sensor Kit:
Store the Sensor Kit between 36°F and 82°F. Storage outside of this range may cause inaccurate Sensor glucose readings.
If you suspect that the temperature may exceed 82°F (for example, in an un-airconditioned home in summer), you should refrigerate your Sensor Kit. Do not freeze your Sensor Kit.
Store your Sensor Kit in a cool, dry place. Do not store your Sensor Kit in a parked car on a hot day.
Store the Sensor Kit between 10-90% non-condensing humidity.
When not to use the System:
Do NOT use if the Sensor Kit package, Sensor Pack, or Sensor Applicator appear to be damaged or already opened due to risk of no results and/or infection.
Do NOT use if Sensor Kit contents are past expiration date.
Do NOT use if the Reader appears to be damaged due to risk of electric shock and/or no results.
What to know before you Apply the Sensor:
The Sensor Pack and Sensor Applicator are packaged as a set (separately from the Reader) and have the same Sensor code. Check that the Sensor codes match before using your Sensor Pack and Sensor Applicator. Do not use Sensor Packs and Sensor Applicators with different Sensor codes together as this will result in incorrect glucose readings.
Wash application site on the back of your upper arm using a plain soap, dry, and then clean with an alcohol wipe. This will help remove any oily residue that may prevent the Sensor from sticking properly.
Allow site to air dry before proceeding. Carefully preparing the site according to these instructions will help the Sensor stay on your body for the full 14 day wear period and help prevent it from falling off early.
Clean hands prior to Sensor handling/insertion to help prevent infection.
Change the application site for the next Sensor application to prevent discomfort or skin irritation.
Only apply the Sensor to the back of the upper arm. If placed in other areas, the Sensor may not function properly.
Select an appropriate Sensor site to help the Sensor stay attached to the body and prevent discomfort or skin irritation. Avoid areas with scars, moles, stretch marks, or lumps. Select an area of skin that generally stays flat during normal daily activities (no bending or folding). Choose a site that is at least 1 inch away from an insulin injection site.
When is Sensor Glucose different from Blood Glucose:
Physiological differences between the interstitial fluid and capillary blood may result in differences in glucose readings between the System and results from a fingerstick test using a blood glucose meter.
Differences in glucose readings between interstitial fluid and capillary blood may be observed during times of rapid change in blood glucose, such as after eating, dosing insulin, or exercising.
What to know about X-Rays:
The Sensor should be removed prior to exposing it to an X-ray machine. The effect of X-rays on the performance of the System has not been evaluated. The exposure may damage the Sensor and may impact proper function of the device to detect trends and track patterns in glucose values during the wear period.
When to remove the Sensor:
If the Sensor is becoming loose or if the Sensor tip is coming out of your skin, you may get no readings or unreliable readings, which may not match how you feel. Check to make sure your Sensor has not come loose. If it has come loose, remove it, apply a new one, and contact Customer Service.
If you believe your glucose readings are not correct or are inconsistent with how you feel, perform a blood glucose test on your finger to confirm your glucose. If the problem continues, remove the current Sensor, apply a new one, and contact Customer Service. Customer Service is available at 1-855-632-8658 7 Days a Week from 8AM to 8PM Eastern Standard Time.
What to know about the Reader’s Built-in Meter:
The FreeStyle Libre 2 Reader has a built-in blood glucose meter that is designed to be used only with FreeStyle Precision Neo blood glucose test strips and MediSense Glucose and Ketone Control Solution. Using other test strips with the Reader’s built-in meter will produce an error or cause the Reader’s built-in meter to not turn on or start a test. The Reader’s built-in meter does not have ketone testing functionality.
The Reader’s built-in meter is not for use on people who are dehydrated, hypotensive, in shock, or for individuals in hyperglycemic-hyperosmolar state, with or without ketosis.
The Reader’s built-in meter is not for use on neonates, in critically-ill patients, or for diagnosis or screening of diabetes.
See Using the Reader’s Built-in meter section for additional important information on the use of the Reader’s built-in meter.
Where to charge your Reader:
Be sure to select a location for charging that allows the power adapter to be easily unplugged. Do NOT block access to the charger due to the potential risk of electrical shock.
Interfering Substances
Taking ascorbic acid (vitamin C) supplements while wearing the Sensor may falsely raise Sensor glucose readings. Taking more than 500 mg of ascorbic acid per day may affect the Sensor readings which could cause you to miss a severe low glucose event. Ascorbic acid can be found in supplements including multivitamins. Some supplements, including cold remedies such as Airborne® and Emergen-C®, may contain high doses of 1000 mg of ascorbic acid and should not be taken while using the Sensor. See your health care professional to understand how long ascorbic acid is active in your body.
BINAXNOW AND ID NOW
ID NOW COVID-19 and BinaxNOW COVID-19 Ag Card have been authorized by FDA under an EUA (and have not been FDA cleared or approved) for use by authorized laboratories only for the detection of nucleic acid or proteins from SARS-CoV-2, and not for any other viruses or pathogens. These tests are only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of in vitro diagnostics for detection and/or diagnosis of COVID-19, under Section 564(b)(1) of the Act, 21 U.S.C. § 360bbb-3(b)(1), unless the authorization is terminated or revoked sooner.
AMPLATZER PICCOLO OCCLUDER
INDICATIONS AND USAGE The AMPLATZER Piccolo™ Occluder is a percutaneous, transcatheter occlusion device intended for the nonsurgical closure of a patent ductus arteriosus (PDA). CONTRAINDICATIONS • Weight < 700 grams at time of the procedure • Age < 3 days at time of procedure • Coarctation of the aorta • Left pulmonary artery stenosis • Cardiac output that is dependent on right to left shunt through the PDA due to pulmonary hypertension • Intracardiac thrombus that may interfere with the implant procedure • Active infection requiring treatment at the time of implant • Patients with a PDA length smaller than 3 mm • Patients with a PDA diameter that is greater than 4 mm at the narrowest portion WARNINGS • This device was sterilized with ethylene oxide and is for single use only. Do not reuse or re-sterilize this device. Attempts to resterilize this device can cause a malfunction, insufficient sterilization, or harm to the patient. • Do not use the device if the sterile package is open or damaged. • Use on or before the last day of the expiration month that is printed on the product packaging label. • Patients who are allergic to nickel can have an allergic reaction to this device. • Prepare for situations that require the removal of this device. Preparation includes access to a transcatheter snare kit and an on-site surgeon. • Accurate measurements of the ductus are crucial for correct occluder size selection. • Do not release the occluder from the delivery wire if either a retention disc protrudes into the pulmonary artery or aorta; or if the position of the occluder is not stable. • Remove embolized devices. Do not remove an embolized occluder through intracardiac structures unless the occluder is fully recaptured inside a catheter. PRECAUTIONS • This device should be used only by physicians who are trained in standard transcatheter techniques. Determine which patients are candidates for procedures that use this device. • The physician should exercise clinical judgment in situations that involve the use of anticoagulants and antiplatelet drugs before, during, and/or after the use of this device. • Patients should have an activated clotting time (ACT) of greater than 200 sec prior to device placement, unless the patient has a significant risk for bleeding and is unable to be anti-coagulated. • The device may be delivered via an anterograde (venous) or a retrograde (arterial) approach. However, in small infants (≤2 kg), the device should be delivered using the anterograde (venous) approach since small infants are at an increased risk for arterial injury. • The AMPLATZER Piccolo™ Occluder contains nickel-titanium alloy, which is generally considered safe. However, in vitro testing has demonstrated that nickel is released from this device for a minimum of 60 days following implant. Patients who are allergic to nickel may have an allergic reaction to this device, especially those with a history of metal allergies. Certain allergic reactions can be serious; patients should seek immediate medical attention if there is suspicion of an allergic reaction. Symptoms may include difficulty in breathing or swelling of the face or throat. While data are currently limited, it is possible that some patients may develop an allergy to nickel if this device is implanted. • Use in specific populations n Pregnancy — Minimize radiation exposure to the fetus and the mother. n Nursing mothers — There has been no quantitative assessment for the presence of leachables in breast milk. • Store in a dry place. • Do not use contrast power injection with delivery catheter. POTENTIAL ADVERSE EVENTS Potential adverse events that may occur during or after a procedure placing this device include, but are not limited to: • Air embolus • Allergic dye reaction • Allergic drug reaction • Anesthesia reactions • Apnea • Arrhythmia • Bacterial endocarditis • Bleeding • Cardiac perforation • Cardiac tamponade • Chest pain • Device embolization • Device erosion • Death • Fever • Headache/migraine • Hemolysis • Hematoma • Hypertension • Hypotension • Infection • Myocardial infarction • Palpitations • Partial obstruction of aorta • Partial obstruction of pulmonary artery • Pericardial effusion • Pericarditis • Peripheral embolism • Pleural effusion • Pulmonary embolism • Re-intervention for device removal • Respiratory distress • Stroke • Thrombus • Transient ischemic attack • Valvular regurgitation • Vascular access site injury • Vascular occlusion • Vessel perforation
CAUTION: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use, inside the product carton (when available) or at eifu.abbottvascular.com or at medical.abbott/manuals for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. ™ Indicates a trademark of the Abbott group of companies. ‡ Indicates a third-party trademark, which is property of its respective owner.